


Great for Lawyers, Not So Great For Everybody Else
An In-Depth Conversation with Attorney Doug Aldeen about Health, Healthcare and Public Health in the United States | By Kimberly J. Soenen | March 8, 2022


(United States Healthcare Refugees. Remote Area Medical Clinic, Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
“Hospitals are really unregulated utilities. We need a national plan that covers everybody. “
-Doug Aldeen
Lawyers are hard to catch.
Billable hours are sometimes tracked at the absurd rate of tenths of an hour. Their professional lives are rooted in the Letter of the Law, rather than the often-times less linear, gray and less analytical areas of the human experience.
Doug Aldeen is an ERISA attorney who recently served as ERISA counsel on behalf of the Berkeley Research Group in New York City to the $7.7 billion May 2016 acquisition of Multiplan and its medical bill repricing product, Data Isight, by the Private Equity firm Hellman and Friedman.
Since 1997, he has represented reference base pricing organizations, a bundled payment software platform, PPO networks, medium to small self-funded plans, TPA’s and provider sponsored HMO’s in various capacities including Herdrich v. Peagram which was argued before the United States Supreme Court in 2001.
He currently serves as a resource to national journalism organizations regarding issues of healthcare and, in addition, as a consultant with the Governmental Relations Committee at the Self Insured Institute of America in Washington D.C. and as an advisor to RIP Medical Debt, which has abolished more $1.2 billion in personal medical debt for financially-distressed Americans who are unable to afford healthcare.
What does all of that mean to a non-lawyer?
Doug and I had an in-depth conversation via email to discuss commercial health insurance industry talking points, Denial of Care vernacular, the ever-snowballing fraud and criminality across the United States Medical Industrial Complex, and why nobody in the United States knows what their medical bill will be until after they are financially distressed or bankrupt.
I disrupted his billable hours mode for one week to talk about the state of health, healthcare and Public Health, from his legal perspective.
Nothing was off the table.

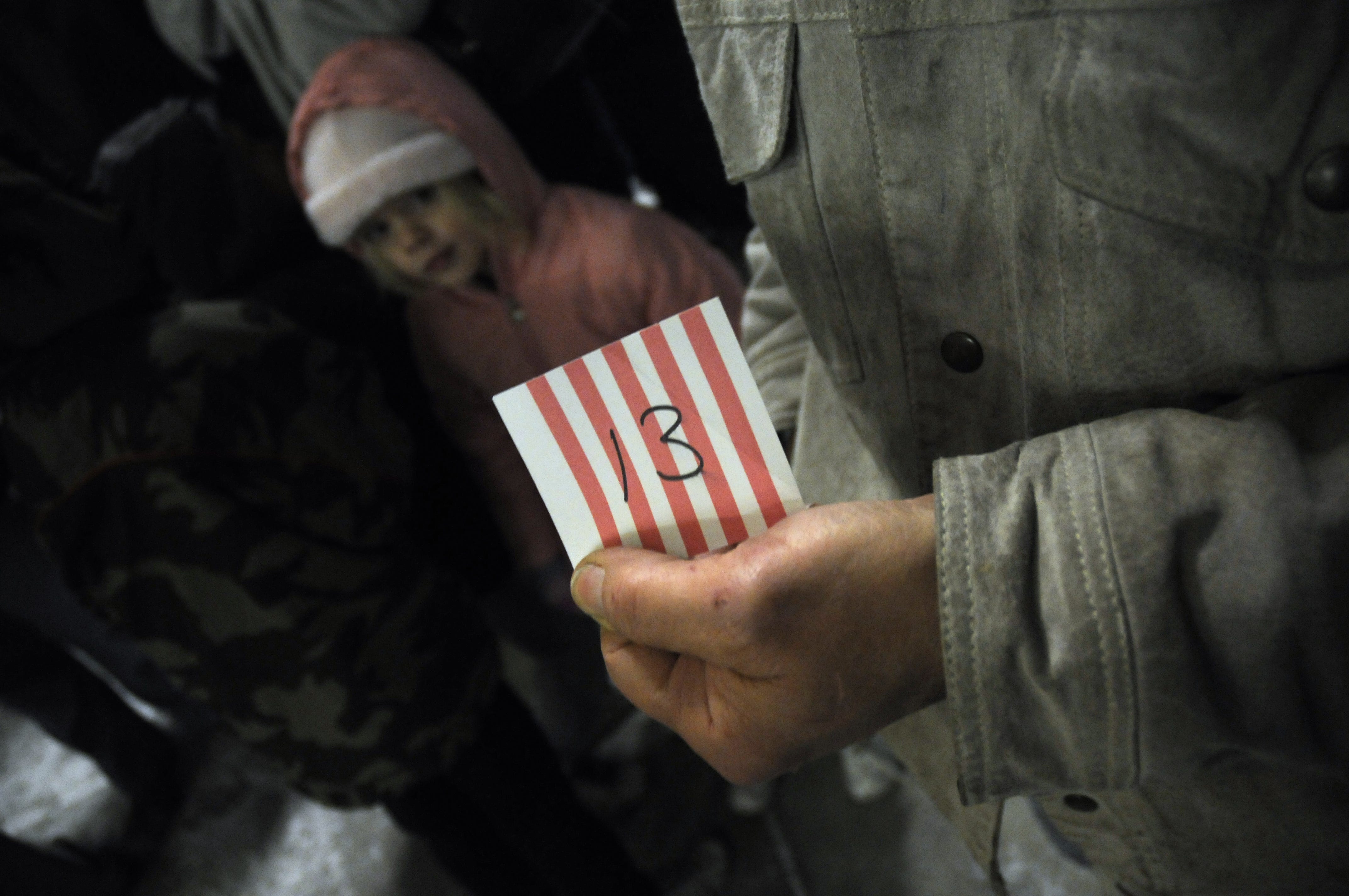
(United States Healthcare Refugees waiting in line in the middle of the night to access the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Persons drive for days to access these temporary conflict-zone triage-type clinics for healthcare. They take a number, and wait. Photo by Dermot Tatlow.)
Where are you from, where do you live, and what is your professional role in the United States healthcare ecosystem?
I am from Urbana, Illinois. Urbana was fantastic place to grow up. It was like living in Mayberry in the 1970’s. I now reside in Austin, Texas, and I am an attorney. I work exclusively in the ERISA health and the United States welfare market (The Employee Retirement Income Security Act of 1974.)
Since 2007, you have operated your own law firm exclusively serving the self-funded industry. What is the “self-funded” industry and how does it differ from your role as general counsel on staff internally with another company?
I serve as outside general counsel to a number of smaller companies. They pay me a retainer monthly. Otherwise, I have a stable of ten to twelve clients that I tremendously enjoy working with daily.
Why did you enter the United States healthcare industry field in 1997?
Great question: The partner at the insurance defense firm left to go to another firm. I had to find another job, as well. It just so happened that the local HMO (Managed Care Health Maintenance Organization) was looking for an attorney.
For those who are not aware, what is the origin of your compensation?
I am compensated typically on a monthly retainer with the ability to participate with a percentage of savings.

(United States Healthcare Refugees wait for healthcare at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Persons take a number and wait for vision, dental and Primary Care hoping to be seen before the free clinic moves on to another distressed area in the United States. Photo by Dermot Tatlow.)
You were once a felony public defender and a litigation associate at an insurance defense firm. Can you tell us more about your experience as a public defender and what specifically is “an insurance defense firm?"
I loved being a felony public defender. I tried five cases and lost every single trial. The lesson: You cannot pick your clients.
More importantly, it was an accelerated education in humanity.
Working at an insurance defense firm means that liability carriers hire the firm to defend the carrier in the event one of its insured cause a car accident. It is soul-killing work that is billed at tenths of an hour.
It is great if you eat at the top of the firm and collect money from the work of others.
In the context of Criminal Defense Law in the United States, clients are appointed legal counsel if they cannot afford private representation. In the context of the United States corporate healthcare industry, however, White Collar criminals generally do have the financial resources to hire a “high-powered” corporate lawyer and “work the system” through back-channel deals to consistently evade incarceration. So, there are very few healthcare industry White Collar crime cases that make it to trial. Most are settled out of court.
Public defenders usually defend one person for one criminal offense. In recent years, healthcare fraud has escalated sometimes including hundreds and thousands of implicated persons who perpetuate healthcare fraud and harm working as a codependent, unethical, complicit system.
For example, in 2020, the United States Department of Justice Criminal Division announced a historic nationwide enforcement action involving 345 charged defendants across 51 federal districts, including the Eastern District of Texas.
In conjunction with the takedown, the CMS (Centers of Medicare & Medicaid Services) Center for Program Integrity announced that it has taken a record-breaking number of administrative actions related to telemedicine fraud, revoking the Medicare billing privileges of 256 additional medical professionals for their involvement in telemedicine fraud schemes.
These defendants—more than 100 doctors, nurses and other licensed medical professionals—have been charged with submitting more than $6 billion in false and fraudulent claims to federal healthcare programs and private commercial health insurance companies, including more than $4.5 billion connected to telemedicine, more than $845 million connected to substance abuse treatment facilities, or “sober homes,” and more than $806 million connected to other healthcare fraud and illegal opioid distribution schemes across the country.
It is worth mentioning that Healthcare White Collar crime is extremely costly for United States taxpayers. Enforcement is led and coordinated by the Department of Justice (DoJ) Criminal Division, the DoJ Healthcare Fraud Unit, Healthcare Fraud and Regional Prescription Opioid Strike Force programs, U.S. Attorneys’ Offices, HHS-OIG, FBI, DEA and others. All are taxpayer-financed accountability bodies.
Over the last two decades, what legal cases have surprised you for the scope and scale of harm and number of willing participants? Can you name a few cases for our readers?
The list is exhaustive and endless. White Collar Crime in the healthcare arena “pays” with little to no recourse. The money at issue is significant and the criminal perpetrators have the majority of it.

(United States Healthcare Refugees wait to access healthcare at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
Over the last 22 years, False Claims, Kick-Backs, Over-Billing Schemes. Price-fixing, Price-gauging and other healthcare fraud schemes have snowballed as industry lobbyists write the laws on Capitol Hill that protect the United States Medical Industrial Complex from being held accountable for their unethical and criminal practices. The Partnership for America’s Health Care Future is the dark money lobbying group that leads that process.
To name a few historic fraud cases: Senator Bill Frist and his family (Columbia/HCA Medicare Fraud), former Florida Governor Rick Scott (HCA Medicare Fraud), Philip Esformes (Medicare and Medicaid Fraud), Mohamed Mokbel, (Pharmaceutical industry fraud) and the entire Sackler-Perdue ecosystem, among countless others.
The CEOs and executive board members of HCA, Cigna, Anthem, Aetna, Centene, UnitedHealth, McKinsey and Company, CVS, Humana and Health Care Service Corporation rarely, if ever, seem to be incarcerated for their crimes.
Why?
Like it or not, in the United States, money can solve many of the defendant’s problems.
Outside of financial incentives, what cases have you worked on that you were most proud of, and why? Lawyers are required to check their emotions and political beliefs at the door. What is the most rewarding aspect of your work with your clients?
I created a new market for resolving claims with hospitals by leveraging financial assistance and paying a fair price. Not-for-Profit hospitals have to provide Free Care to both uninsured and underinsured patients for all “medically-necessary” and “Emergency Care” services solely based upon income because half of United States residents and citizens earn less than $35,612 annually per household.
What was Herdrich v. Peagram and what influence did that decision have on your career path?
The Herdrich case was an ERISA case that gained national traction as the HMO became an unpopular acronym. It was a watershed moment that allowed me access to the top law firms in the country and gave me the opportunity to make some great connections.
What did the case achieve to better Public Health or strengthen Public Trust?
Truthfully, Herdrich did not advance anything in terms of strengthening Public Trust. It was case solely based upon misaligned incentives and denial of care. All it really did was continue to refine the area of ERISA law and how to assert claims.
Great for lawyers, not so great for everybody else.


(United States Healthcare Refugees receive dental care from volunteer dentists at the Remote Area Medical Clinic, Leburn, Kentucky, 2009. RAM is supported entirely by private donations in an effort to close the Death Gap in rural America. For some, this is the only dental care they can access within hundreds of miles of their homes. Photo by Dermot Tatlow.)
In your ten years working inside healthcare provider-sponsored HMOs in both Champaign-Urbana and San Antonio, Texas as an Associate general counsel and general counsel, what cases and experiences with clients most influenced your thinking about healthcare access in the United States?
The sheer amount of money that flows in and out of a commercial health insurance company and the inherent conflicts and misaligned incentives that exist in healthcare.
In the 1990’s, Managed Care started to accelerate its lobbying power on Capitol Hill and erected countless barriers to accessing healthcare for The Patient. Terms like “In-Network,” “Pre-existing Condition,” “Medical Loss Ratios,” “Benefit Buy Downs,” “Co-Pays,” “Co-Insurance,” “Pre-authorizations,” “Denied Claim,” “Appealed Claim,” “Retroactive Emergency Room Denial,” and other terms were drafted by the commercial health insurance industry to support Denial of Care as their national industry business model.
Can you talk a little about the legal language of Denial of Care for profit?
When an insurance carrier, such as UnitedHealth, which is a publicly traded entity, bears the full risk for payment for medical services, the REAL master United serves is not the policy holder but rather its shareholders. In other words, there is an incentive to “keep” dollars in-house rather than pay claims.
Americans like to trumpet “choice” as consumers, and “freedom” as participants in the competition-driven United States healthcare model, and yet, the paradox—the embarrassing irony—is they have absolutely no choice, none, in their healthcare.
70 percent of healthcare services are involuntary, such as a heart attack, breaking your leg skiing, etc. How can there be “choice” when an individual is either in pain, or under the influence of pain narcotics? By its very definition, there is no arm’s length transaction for the majority of services. Does that give the physician or hospital the right to price-gauge?
There is that context, yes. Also, if persons want to select a commercial health insurance company, a health insurance plan and medical professionals of their own choosing, they cannot. They are pooled into the Affordable Care Act (ACA) and only able to select “coverage” from a very restricting and limited options.
Or, if persons are employed, they have to become a member of the commercial health insurance provider their employer selects for them. Once “insured,” they cannot choose their own network of medical professionals, their medicine, their lab, their physicians, their clinic or their own surgeon. And, they often are not covered for vision, dental, preventive or holistic care.
If you are disabled, it’s an entirely different administrative nightmare ridden with barriers to care.
On the other side, wealthy persons can select Concierge Physicians and pay out of pocket for any physician, hospital or medical professional they choose.
Is not having a choice healthy?
Not having any choice is not healthy.
In fact, tying commercial health insurance coverage to employment is even worse both for the employer and the employee. Why does an employer want to pay for somebody’s health issues and why would an employee want to be “stuck” in a job solely for the health benefits?
It is a model that needs substantial change.

(United States Healthcare Refugees receive dental care from volunteer dentists at the Remote Area Medical Clinic, Leburn, Kentucky, 2009. For some adults, a visit to RAM is the first time they have ever received dental care. Dental care in the United States is rarely covered by commercial health insurance. Photo by Dermot Tatlow.)
Has Managed Care worked to leverage Public Health and improve the health of United States citizens, residents and business owners?
Absolutely not.
There is no money in “good health.”
I do believe there is a significant component to personal responsibility and maintaining good health.
And yet, chance, circumstance and luck—what you call “involuntary” healthcare needs—is the reality.
Nobody knows when, or if, they will be injured, become ill, become disabled or die. Persons can minimize risk through “personal responsibility” or “maintaining good health,” but the factory worker in Texas who has worked on the manufacturing line for 25 years and gets injured on the job may argue with the “responsible-living” premise.
The Spinal Cord Injury victim who was paralyzed in a car accident at the age of 13 while riding in the back of her family’s station wagon may not agree with the presumptive responsibility premise. Nor will the non-smoking vegan who gets cancer, the NCAA Division 1 scholarship athlete who gets multiple sclerosis, or the husband who gets at amyotrophic lateral sclerosis at the age of 31.
There is also the parent of the seven-year-old son who gets bone cancer who may not agree that '“being responsible” guarantees good health.
That said, what has been the most difficult thing to witness since 1997 as people bring cases to you?
Not-for-Profit hospitals suing individuals whom they know cannot afford their healthcare services instead of fulfilling their charitable mission.
It is a dysfunctional model that is a “death trap.”
You get sick, need help, and then get sued because you are upside down, meaning, perhaps cannot work as a result of the injury, illness or disability and simply cannot keep up with the bills.

(Two police officers talk in the field nearby the Remote Area Medical Clinic for United States Healthcare Refugees in Leburn, Kentucky, 2009. Persons drive for days to access healthcare at this conflict-zone triage-type temporary clinic. Police offer security as hundreds of persons flood the clinic and wait for care over night in their cars in dangerous winter temperatures. Photo by Dermot Tatlow.)
What are some examples of legal health-related cases you hear about in your circles that you cannot imagine occurring to your own family?
“Pill mills.”
I cannot imagine a physician over-prescribing an opioid to a member of my family knowing how addictive it is, solely based upon financial incentives.
The Sackler family (Perdue Pharmaceuticals) were paid handsomely and simply “bought” the United States Department of Justice and Attorneys General, paid a fine, and discharged all the families in bankruptcy that were destroyed by their actions.
The most difficult thing to witness over the past 25 years is how medical debt has become pervasive and reaches into every corner of society solely because people get sick or injured.
Let’s talk about that medical debt.
Americans shoulder as a result of cost-shifting to The Patient by Managed Care and the hyper-inflated medical bills the industry charges at every corner. There is upwards of $88 billion in medical debt among people in the U.S., a March 2022 Consumer Financial Protection Bureau report has found. There is $88 billion in medical debt on consumer credit records since June 2021, but this amount is likely higher because not all medical debts are sent to consumer reporting companies.
Medical debt is the most common debt collection tradeline on credit records, accounting for 58 percent of all third-party debt collection tradelines as of 2021. Medical debt reported to consumer reporting companies that are past due can end up on credit reports and lower credit scores, making it harder to find a job or home.
Black and Hispanic people, young adults, low-income people, veterans and older adults are disproportionately affected by medical debt. People in the Southeastern and Southwestern United States are also more affected by medical debt.
Because medical bills vary and are unpredictable, uninsured and out-of-network patients typically are charged more than in-network patients. Often these charges to uninsured and out-of-network patients are higher than providers' costs.
You advise RIP Medical Debt on certain deals as a lawyer. For readers who are not aware, what is RIP and how does RIP select candidates for medical debt forgiveness? Does any entity or group of individuals benefit financially from this process?
RIP Medical “buys” medical debt on the secondary market for less than a penny that typically pays off $10,000 in “debt.” RIP serves as the “broker.” If a person, and when a church, as an example, wants to pay $10,000 of debt off, RIP will go into the market and buy with their money, $10 million in medical debt for $10,000 and “poof” it is gone.

(United States Healthcare Refugees receive dental care, vision care and medical care from volunteer medical professionals at the Remote Area Medical Clinic in Leburn, Kentucky in 2009. Persons are directed to take a number, and hope to get seen at the temporary conflict-zone triage-type clinic. Photo by Dermot Tatlow.)
In your ten years working inside healthcare provider-sponsored HMOs in both Champaign-Urbana and San Antonio, Texas as an associate general counsel and general counsel, what were the most common cases to surface and what were some of the cases that most impacted you or influenced your thinking about healthcare access?
The sheer amount of money that flows in and out of a health insurance company and the inherent conflicts and misaligned incentives that exist in healthcare.
Can you name a few of the inherent conflicts and misaligned incentives that exist in healthcare on all levels?
A broker that is working for a group BUT is paid by the insurance carrier; Repricing medical bills where the vendor repricing the bills makes more in a fee than the medical provider providing the services; Fee-for-Service arrangements in healthcare that encourage ordering more tests; This topic requires a book….
Will you write that book?
I will write that book someday.

(Across the U.S., 136 rural hospitals and clinics have closed since 2010, and more than 21 since 2020, according to the Cecil G. Sheps Center for Health Services Research. Here, United States Healthcare Refugees wait for healthcare access at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
As Private Equity moves in hard and fast like vultures on the distressed and buckling United States healthcare and hospital industry, what has your experience been with Private Equity firms purchasing Long Term Care Facilities, buying up distressed hospital assets and working in commercial health insurance?
Private Equity is a very lucrative way to earn a living in healthcare since there is no uniformity in price. You can charge whatever you can collect. There is an entire subreddit column that we could devote this topic.
We see a lot of executive board movement where hedge fund executives are now sitting on commercial health insurance boards, hospital boards and other governance bodies in the healthcare industry. Is this cross-pollination healthy for Best Practice, Quality of Care, Patient Safety and Fear-of-Reprisal Free work environments?
You cannot serve two masters: It’s money or patients.
The bottom line is that we live with a sick Medical Industrial Billing Complex that rewards hospitals not for Preventative care, but after the fact that the patient has become a Type 2 Diabetic.
What is SIIA and what governmental relations committee and price transparency work have you done?
I work with members of United States Congressional staff to help guide and develop regulations for price transparency.
How is that going? Do you, personally, know what the cost of healthcare will be for your employees, family and you month-to-month?
The United States needs a “market” for healthcare to bring the prices down.
As an example, the Lasik eye surgery started out at roughly $3000.00 per eye, and now I think this can be done for $600.00.
For services that are “involuntary” (illness, injury, disability, etc.) we need a system that will cover those situations.
You can have a “tax supported” lawyer (public defender) in the event you cannot afford one, at a minimum, so we should do the same so individuals do not become insolvent solely because they make the mistake of having a heart attack or becoming ill, injured or disabled.

(A young United States Healthcare Refugees receives dental care at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. For many, this is their first time receiving dental care. The white sugar epidemic impacts dental health disproportionately in southern states. Photo by Dermot Tatlow.)
You won the 2020 Shkrelli Award from the Lown Institute for your submission regarding Not-for-Profit hospital balance billing practices. So many hospitals have Not-for-Profit status and yet their Executive Management-to-Staff Pay Ratios are astonishingly off-kilter.
For readers who are not well versed in the tax status of Not-for-Profit hospitals in the United States, why are some hospitals allowed that status and others not?
This is my passion.
Anybody can establish a “Not-for-Profit” (NFP) hospital but the basis is the existence of a charitable endeavor.
What is the difference between a NFP Hospital and For-Profit Hospital?
The profit motive is the difference, legally. The real deal is that NFP’s are more profitable than their counterparts.
How are their governing bodies different, if at all?
Shareholders vs. Members of the Community. But the reality is there is no difference.
Upon what criteria is NFP based and how do hospitals qualify for NFP status?
The IRS grants the NFP status. But like most things the government does, it does a terrible job policing…
Is there a Charity Care annual financial minimum allocation for NFP Hospitals?
No. The hospitals set up the system that way.
Are their salary caps for the CEOs of NFP hospitals?
No.
Can For Profit hospitals accept shareholder, donor or other investor money that NFP Hospitals cannot by law?
Absolutely. Heads in beds. Hand people cheeseburgers and cigarettes. And just sit back and start collecting their money.
This is a white-hot topic now. Tell readers more. Why aren’t all hospitals For Profit? Why aren’t all hospitals Not-for-Profit? Explain.
We simply need enforcement of a hospital’s charitable endeavor. There needs to be an established level of charity care that is, at a minimum, commensurate with the amount of tax breaks received.

(A physician directs United States Healthcare Refugees as they wait for healthcare access at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
In 2019, before the pandemic, pressure to rein in healthcare costs did not reach hospital executive suites, where spending on CEO pay is rising sharply. Top executives at six of the nine largest Chicago-area Not-for-Profit health systems pocketed substantial raises in 2017. Their average pay hike was 37 percent, easily outpacing national trends in other professional fields.
The C-Suite at Cook County Health System in Chicago has frequently received D and F ratings on Patient Safety and their turnover is astonishing.
Jim Skogsbergh, of Advocate Aurora Health, was the highest-paid local CEO for the fifth year in a row, taking home $11.7 million in 2017—up 42 percent from the year prior. He received more than twice as much as Dean Harrison of Northwestern Memorial Healthcare, the second-highest-paid CEO, who collected $5.2 million—up 22 percent from 2016.
In many cases, pay hikes were driven by bonuses based on "performance targets" that reflect the broader push for greater “efficiency" and better patient care.
What, by your definition does “efficiency” in hospitals mean? And what are your thoughts on the pay disparity between hospital CEOs and medical professionals working in Primary Care, Social Work, Emergency Medicine, Nursing and Intensive Care Units?
Heads in the beds. Hospitals need patients. “Efficiencies” as mentioned above is really billing efficiency and increasing revenue.
And, for those who do not understand the United States model of healthcare, how do United States hospitals “increase revenue?”
Increase their “Charge-master” and “Upcode” (over-bill) the services they provide.
The number of whistleblowers in healthcare have increased since the dawn of Managed Care in the 1990’s. A Medicare Fraud Strike Force was set up by President Obama years ago, and yet, the fraud and criminality across United States healthcare industry is astonishing by any economic metric or ethics measure.
Let’s talk about upcoding, False Claims and billing fraud. What kind of fraud increases have you witnessed as a lawyer in the last 30 years and has the type of fraud changed?
Upcoding is the biggest fraud perpetrated in healthcare. Upcoding is the single biggest factor right now in revenue streams for hospitals.
As an example, how can you go from 80 percent of ER visits that were level 1 two years ago, to 80 percent of level 3 ER visits in the EXACT same market with the EXACT same mix of patients simply because there was acquisition by another health system?
Readers often see “False Claims” (methodical over-billing) cases by the Department of Justice where commercial health insurance companies are charged with criminal activity but settle those crimes out of court with a payout to the Department of Justice. “False Claims” is White Collar Healthcare billing fraud.
This can be upcoding, over billing, duplicate billing and an array of other tactics major corporate health systems utilize that distress patients financially and emotionally. But over-billing is not a pandemic-caused phenomena. This dates back to the dawn of Managed Care in the 1990’s.
In February of 2008, the New York Office of the Attorney General began conducting and commercial health insurance industry-wide investigation into a scheme by commercial health insurers to defraud consumers by manipulating reimbursement rates and upcoding across all of their databases.
At the center of the scheme was a company called Ingenix, Inc., the nation’s largest provider of healthcare billing information at the time, and it served as a conduit for rigged data to the largest commercial health insurance companies in the country. In short, the company rigged their data to over-bill systemically, consistently for UnitedHealth and other commercial health insurance company clients.
Columbia/HCA and countless others have been indicted over the last 25 plus years for over-billing yet no executives are convicted or incarcerated.
How do we legally end that healthcare industry scam and hustle?
It is two-fold: Government strong arming certain aspects such as buying ALL drugs coupled with private initiatives.
What is Monopsony with Epic and Cerner and why do two companies dominate the Electronic Medical Records field? We are a tech capital of the world. It seems there would be more players and more competition in a United States “free-market” scape?
The “cost” of getting into the game is prohibitive.
As Private Equity moves in hard and fast like vultures on the distressed and buckling United States healthcare and hospital industry, what has your experience been with Private Equity firms purchasing Longterm Care Facilities, buying up distressed hospital assets and working in commercial health insurance?
Private equity is a very lucrative way to earn a living in healthcare since there is no uniformity in price. You can charge whatever you can collect. There is an entire subreddit column that we could devote this topic.
Let’s go deeper.
What happens when a Private Equity firm buys a hospital, a Longterm Care Facility, hospital chain, or cross-pollinates with a commercial health insurance company? How do those firms and their shareholders profit from illness, injury, disability and death? It’s a difficult concept to comprehend morally and ethically.
There is no money in health.
The sicker you are and “well insured,” the more profitable the healthcare enterprise, especially when you can set your own price and there are no market dynamics. Private Equity firms make a ton in this space because they are buying streams of revenue. We could discuss this for hours.
Is there value in health in keeping the United States work force competitive, healthy and able-bodied by removing barriers to healthcare access? Is it possible to assign value to health, not as a commodity, but as a foundational cornerstone of international competitiveness? The burden of poor American Public Health seems to cost tax payers dearly.
Forward thinking countries in Europe and Latin America take this approach. We are literally killing our citizens both financially and physically, for profit.
We see a lot of executive board movement now where Hedge Fund executives are now sitting on commercial health insurance boards, hospital boards and other governance bodies. Is this cross-pollination healthy for Best Practice, Quality of Care and Patient Safety?
You cannot serve two masters: It is money or patients. The bottom line is that we live with a medical sick industrial billing complex that rewards hospitals not for preventative care but after the fact that the patient is a type 2 diabetic.
Ah yes, the factory healthcare trend. Treat em’ and Street em’.
Americans have been told they have the best healthcare system in the world, and yet, our health outcomes and health ratings globally—by all indicators—illustrate how unhealthy a country the United States is.
Heart disease, diabetes, obesity, diabetes, suicide rates, depression, violence, anorexia, cancer…there’s a disconnect there between The American Myth and the reality. For example, rural hospitals are closing, city hospitals are going bankrupt, Patients are delaying care for many reasons (mostly cost) and Remote Area Medical clinics are taking care of United States Healthcare Refugees with conflict-zone triage-type healthcare across the United States on a weekly basis.
While this is happening, many corporate health systems and commercial health insurance companies are expanding overseas in Doha, Ryad, Qatar, London, UAE and other countries and raking in record-breaking profits. Where does that money for investment overseas come from?
Good question. I do not know the answer to that one.
What is SIIA and what governmental relations committee and price transparency work have you done?
I work with members of congressional staff to help guide and develop regulations for price transparency.
There has been a lot of policy news about this push for price transparency. Can you update us on where it stands in the United States now and how it will benefit patients, families and business owners? What’s the good news?
Price transparency is the law of the land. Unfortunately, hospitals only have a $300.00 per day fee for noncompliance with the law which is $106,200 for the year. It is cheaper to not comply.
The health plans will have the same issue effective July 1, 2022.
But, think IF you had all the prices and could see that cash is the lowest price.
You won the 2020 (Martin) Shkrelli Award from the Lown Institute for your submission regarding Not-for-Profit hospital balance billing practices. So many hospitals have Not-for-Profit status and yet their executive Management-to-Staff Pay Ratio is astonishing and dangerous budget cuts to ICUs, ERs and nursing staffs persist.
But Shkrelli, who was demonized as greedy and self-serving, simply did what the pharmaceutical industry, commercial health insurance industry and nursing agencies have been doing for decades and are doing now, mid-pandemic: Inflating costs irrationally and price-gauging legally.
He was eventually incarcerated on other charges unrelated to legal price-gauging. What’s Un-American or illegal about what he did? That’s the American way, no?
Nothing really. Shkrelli simply saw an opportunity to corner a market but did so with a Cheshire cat like grin. If he would have been more understated and simply flew under the radar, he would be sailing in the Caribbean right now.

(United States Healthcare Refugees wait in the middle of the night, in the winter, for healthcare access at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
Before the pandemic, pressure to rein in healthcare costs was not reaching hospital executive C-Suites, where spending on CEO pay continues to increase sharply each year.
Top executives at six of the nine largest Chicago-area Not-for-Profit health systems pocketed substantial raises in 2017. Their average pay hike was 37 percent, easily outpacing other national industry trends for growth.
The C-Suite at Cook County Health System in Chicago has frequently received D and F ratings on Patient Safety and their staff turnover is exhausting.
Jim Skogsbergh of Advocate Aurora Health was the highest-paid Illinois CEO for the fifth year in a row, taking home $11.7 million in 2017—up 42 percent from the year prior. He got more than twice as much as Dean Harrison of Northwestern Memorial Healthcare, the second-highest-paid CEO, who collected $5.2 million—up 22 percent from 2016. In many cases, pay hikes were driven by bonuses based on "performance targets" that reflect the broader push for greater “efficiencies" and “better patient care.”
What, by your definition does “efficiency” in hospitals mean? And what are your thoughts on the pay disparity between hospital CEOs and frontline medical professionals working in Emergency Medicine and the ICU, for example?
Heads in the beds. Hospitals need patients. Efficiency, as mentioned above, is really billing efficiency and increasing revenue.
For readers who don’t know, how do hospitals increase revenue when it is impossible to predict volume and predict need? Is cutting medical staff, medical supplies and hospital beds “efficient” in order to profit?
Hospitals simply increase their charges. I wish there was more to it than that. It is a game: Charge more for the services that patients utilize and charge not as much for the services patients do not utilize.
What is the mission of the Cedric Benson Foundation that you are involved with?
CBF is a foundation that helps further disadvantaged kids move forward in life.
Please educate readers about MLR and the ACA and the perverse market incentives:
The Affordable Care Act (ACA) requires insurance carriers to pay 80 percent of its premium in claims payments (MLR Rule). The remaining 20 percent is allocated to salaries, bonuses, etc. The perverse market incentive that was created was to INCREASE the size of the pie and instead of having $1 Billion as your 20 percent for salaries, etc. You now have $20 Billion.
Now, for non-lawyers, can you explain that?
Increase the size of the pie and take a bigger share.
Boom. That’s it. That’s a good bridge to the topic of fractured Public Trust.
Public Trust in healthcare, especially in the United States, is frayed and damaged. Some would argue, the fractured trust is beyond repair in the United States because it is a country that politicizes healthcare policy like no other country in the world.
Tell us what changes you think need to be implemented now in the United States approach to, and model of, healthcare to restore trust?
Hospitals are really unregulated utilities. We need a national plan that covers everybody.
70 percent of healthcare interactions are involuntary (I did not choose to have a heart attack, for example) which should not give rise to a medical professional price-gauging you solely because you needed help or got sick.
The Single Payer reform movement in the United States is now in its 183rd year. Grass roots allies and business owners who support Single Payer reform in the United States have never been more organized, vocal or forceful.
Organizations like Business Leaders for Health Transformation, Students for a National Health Program, National Nurses United, Healthcare For All Los Angeles, the newly-launched Minnesota Healthcare for All caucus, and others are all taking action to enact and implement Universal Healthcare at the state and federal levels.
Do you support House Resolution 1976 / The Medicare for All Act of 2021, more commonly known as National Improved Medicare for All?
You can be the worst criminal on the planet and in the United States, you will get a lawyer if cannot afford one. We can do the same in healthcare, as well.
A vague and lawyerly response. Can you be more specific?
There are a ton of smart people in this space that can devise a very fair and fundamental system for all to access.
You are a father of many children. Talk a little about that chance, circumstance and luck you referenced—”involuntary healthcare” vs. “voluntary,” as the industry calls it. Can commercial health insurance companies predict health?
Insurance is about risk. You can gauge risk with information and game the system. I am never surprised by the level of sophistication inside publicly traded insurance carriers. There is a ton of opportunity there.
(Take a number. United States Healthcare Refugees wait for healthcare access at the Remote Area Medical Clinic in Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)
In your opinion, is the United States For-Profit approach to, and model of healthcare, sustainable?
No.
Does the United States have “The best healthcare system in the world?”
No.
Thank you for your time and perspective, Doug.
RECOMMENDED READING
Medical Debt Crisis in the United States Study by Stanford Institute for Economic Policy Research - America’s medical debt has been widely tagged as an $81 billion crisis. Americans are actually saddled with at least $140 billion in outstanding medical debt.
INVESTIGATIVE JOURNALISM
March 8, 2022 - A month after a U.S. bankruptcy court signed off on Mallinckrodt’s reorganization plan, the company has agreed to a $260 million settlement to resolve claims by the Department of Justice surrounding its management of its controversial Acthar Gel drug. The U.S. said that Mallinckrodt underpaid Medicaid rebates and used a foundation to pay illegal copay subsidies, violating an anti-kickback statute by inducing patients to use the treatment - By Kevin Dunleavy
The Health Insurance Hustle by ProPublica
How to Make Health Insurers Take Fraud Seriously by ProPublica
Illinois’ $16 Billion Health Program Is Riddled with Industry Ties and Potential Conflicts of Interest - Milking Medicaid: The state health care agency has a revolving door for executives from the insurance industry - By David Jackson
Insurance Firms Reap Billions in Profits While Doctors Get Stiffed for Serving the Poor - Milking Medicaid: State-contracted insurance firms balk at paying frontline medical providers, threatening the viability of leading hospitals and clinics, and imperiling Illinois' entire Medicaid program - By David Jackson and Kara Leadholm
Pritzker Trust Bought Stock in a Top Illinois Contractor After He Was Elected Governor - Purchase of stock highlights weakness of Pritzker’s blind-trust arrangement in preventing conflicts of interest for billionaire governor’s holdings - By David Jackson
LISTENING
ORGANIZATIONS
Business Leaders for Health Transformation
Legal Resources
Department of Justice Healthcare Fraud Unit
EXHIBITIONS
“SOME PEOPLE” (Every)Body digital exhibition at All About Photo Magazine
ABOUT THE PHOTOS IN THIS ARTICLE
United States Healthcare Refugees by Dermot Tatlow
The night was bitterly cold as the temperature dropped to 14 degrees Fahrenheit in the mountains of Eastern Kentucky, where hundreds of cars parked overnight outside the Knott County Sportsplex. Inside the vehicles, families sat huddled, running their engines intermittently for warmth. They planned to be there all night to make sure they got a first- come, first-served ticket to access desperately needed free medical and dental healthcare. Remote Area Medical (RAM) clinic trucks are emblazoned with signs that say, “Disaster Relief.”
Staffed by volunteers, RAM was founded to provide medical services to the most vulnerable people in the developing world. That was, until RAM realized that the most vulnerable also lived in the United States of America, where RAM now provides more than half of its services. RAM’s field hospital setup was originally designed to cater to mass casualties caused by natural disasters in other countries. That was, until they realized that in the United States millions of uninsured and underinsured people are consistently and systemically denied healthcare.
Many uninsured people are workers who hold two—and sometimes three—jobs. Unfortunately, these minimum wage and part-time jobs allow employers to legally avoid providing their employees with medical insurance.
For me, a European photographer who has covered refugees and evacuees from conflicts and natural disasters around the world, I was astonished to see hundreds of American families, with young children in their cars, lined up overnight in freezing conditions to seek the most basic healthcare.
The poem on the Statue of Liberty reads, “Give me your tired, your poor, your huddled masses...” And here, they were huddled still, on a frozen mountain in Leburn, Kentucky.
People are made to take a number in order to access healthcare at the RAM temporary field clinic in Leburn, Kentucky. As relieved as these families are to access medical care on this day, their abiding question is, “What will we do when we need healthcare tomorrow?”
These people have become healthcare refugees in their own country.
(United States Healthcare Refugees. Remote Area Medical Clinic, Leburn, Kentucky, 2009. Photo by Dermot Tatlow.)